The NNI stuff from Charanya:
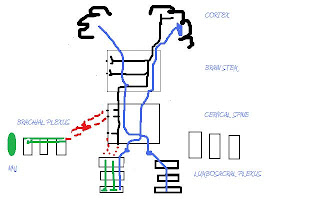
The black tract: corticospinal/pyramidal tract which decussates at the brainstem before synapsing at the anterior horn cells at their respective spinal levels
The blue one: Spinothalamic
Okay case scenario1: Patient comes in for weakness of the biceps
So, is it a NERVE or a NERVE ROOT problem?
Nerve: Musculocutaneous nerve C5-7 (mainly C5)
What other nerves have C5? That will be the axillary nerve (C5, C6)
Which means if its a musculocutaneous nerve problem, deltoids weekness and regimental badge sign will be absent
If its a nerve root problem, then biceps weakness will be accompanied by deltoids weakness (abduction) and regimental badge sign
Case Scenario 2:
If a patient presents:
- flccidity of the LL
- upgoing plantars
The lesion is probably in the conus medullaris where both spinal cord and peripheral nerves exist and may present as such
Case scenario 3:
Patient presented with hemiparesis without facial involvement:
1. Spinal cord or brainstem lesion below level of pons (where CN*VII nerves are)
2. Cortical lesion of motor cortex sparing the region responsible for facial motor (facial nerve UMN)
General Thought Flow:
Patient with right hemiparesis:
Q1: sensory loss on the Left side?
- Yes: spinal cord lesion, Brown Sequard
- No: above
Q2: cranial nerve lesion?
- Yes: brainstem lesion. Gauge the site wrt Cranial nerves involved. Do jaw jerk
- No: higher up or below the level of exiting cranial nerves (e.g. caudal medulla)
Q3: Aphasia, neglect, visual deficits
- Yes: cortical lesion
- No: subcortical or caudal brainstem lesion

